Methods: B etween J anuary 2 019 a nd N ovember 2 023, a t otal o f 58 patients (32 males, 26 females; median age: 4.5 years; range, 8 months to 16 years) who underwent transcatheter closure of ventricular septal defects using the Konar-MF™ device were retrospectively analyzed. Patient demographics, procedural details, and follow-up data were recorded.
Results: Procedural success was achieved in 95% of cases, with a median procedure time of 60 min and fluoroscopy time of 12.6 min. Retrograde implantation was used in 79% of patients, significantly reducing procedural time and minimizing complications associated with an arteriovenous loop. Our refined strategy of selecting smaller devices when anatomically feasible played a crucial role in reducing interference with surrounding cardiac structures, substantially contributing to the absence of complete atrioventricular block in our cohort. Major complications included device embolization, moderate aortic regurgitation due to device dislocation, and right ventricular perforation (each in 1.8% of patients). The median follow-up was 34.5 months. Residual shunt rates were initially 42% on postoperative Day 1, reducing to 1.8% by the end of the follow-up period.
Conclusion: The Konar-MF™ occluder demonstrated high procedural success and acceptable complication rates for perimembranous ventricular septal defect closure. The use of a retrograde approach and a refined device selection strategy were key factors in achieving favorable outcomes, minimizing complications such as atrioventricular block and valve interference. The device offers significant advantages, making it a suitable alternative to surgical ventricular septal defect closure.
In this context, the LifeTech Multifunctional Occluder (Konar-MF™) has emerged as a promising option. Approved by the CE in 2018, this device offers a flexible, hybrid design that allows both antegrade and retrograde deployment through a small sheath. Its unique construction is aimed at minimizing potential damage to surrounding structures and reducing the risk of complications, such as complete heart block. Nevertheless, comprehensive data on the efficacy, safety, and long-term outcomes of the Konar-MF™ device remain limited.
This study aims to evaluate the mid-term outcomes of transcatheter VSD closure using the Konar-MF™ device, with a focus on its effectiveness and clinical relevance. While the device offers several advantages, such as flexible deployment and a reduced risk of complications, it is important to acknowledge the challenges posed by anatomical variations and the learning curve associated with mastering its technique. In the present study, we aimed to uniquely investigate the combined benefits of retrograde approach and tailored device selection, filling a gap in the current literature on pediatric VSD closure.
Device selection
As supported by previous studies[3, 4] and information provided by the manufacturer, for PMVSDs, we initially selected a device where the right ventricular (RV) disk was 1 to 2-mm larger than the measured defect size on the RV side. This approach aimed to ensure complete closure while accommodating potential anatomical variations. Although this sizing strategy was effective in cases with conical defects and sufficient aortic rims, it occasionally led to interference with the aortic valve or tricuspid apparatus. As we gained more procedural experience, we refined our device selection strategy, and in later cases, we typically selected a device size only 0.5 to 1-mm larger than the RV measurement. In some patients with severely deficient aortic rims, we even opted for a device size equal to the RV measurement. This more individualized approach was particularly useful in defects involving septal aneurysms, which often presented with multiple openings on the RV side. In these cases, the width of the aneurysm was carefully considered during device selection to ensure optimal filling while minimizing contact with the heart valves, thereby facilitating the use of smaller devices, even in complex defects. For muscular VSDs, we applied a similar strategy, typically selecting a device size with a 0.5 to 1-mm margin on the RV side, which was sufficient to achieve complete closure while preventing unnecessary extension into adjacent structures.
Interventional procedure
All procedures were performed under general anesthesia or deep sedation, chosen based on patient age, health, and defect complexity, with general anesthesia favored for younger children and longer procedures. Prior to device deployment, a comprehensive assessment of the VSD was conducted to determine the defect"s diameter, morphology, location, and its relationship with critical surrounding structures, such as the aortic and tricuspid valves. In the first three patients, transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) were used to map the defect and plan the closure. For later cases, TTE alone proved sufficient. To further guide the procedure, left ventriculography was performed using precise angiographic angles, tailored to the type of defect being addressed.
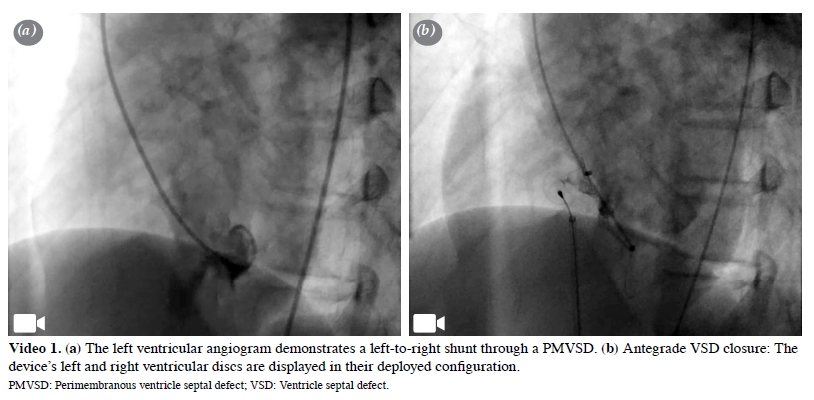
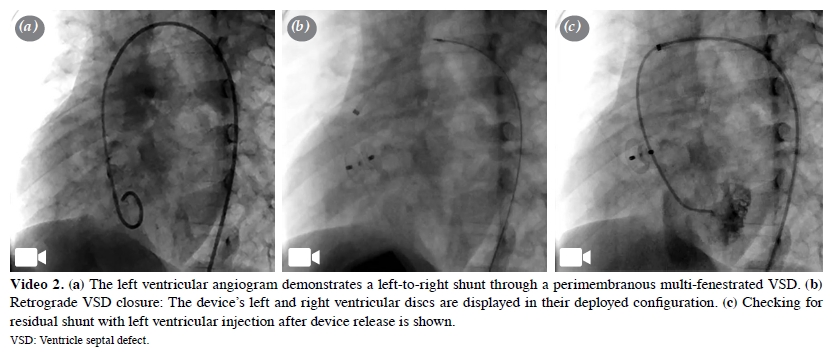
Although the traditional approach for VSD closure has primarily relied on the antegrade route, the Konar-MF™ device"s adaptability for both antegrade and retrograde approaches necessitates a distinct strategy. The retrograde approach, which involves advancing the device from the femoral artery to position it from the LV side of the defect, provides a more direct route and eliminates the need for atrioventricular (AV) loop formation. This approach is preferred for both perimembranous and muscular defects, making the procedure more efficient and straightforward. However, in cases with defects located close to the aortic valve or with mild aortic valve prolapse, the antegrade route can be more advantageous. Additionally, when access from the RV side is favorable, the device can be implanted directly via the antegrade route without the need for AV loop formation. Once the device was positioned, its placement was thoroughly confirmed using TTE before release to ensure that it was appropriately aligned with the defect and that there was no impingement on surrounding structures, such as the aortic or tricuspid valves. After the device was released, additional post-release assessments were conducted using a combination of TTE, left ventriculography, and aortography. Aortography was also employed in some cases to specifically check for any new or worsened aortic regurgitation (Figure 1, Videos 1 and 2).
Follow-up protocol
On the first day after the procedure, each patient underwent a comprehensive evaluation that included a 12-lead electrocardiogram (ECG), echocardiography, and chest radiography. Follow-up visits were scheduled at one, three, six, and 12 months after the procedure. During these visits, repeat ECG and echocardiography were performed. Following the first year, patients continued to undergo annual evaluations, ensuring sustained surveillance for potential late complications.
In cases where early post-procedural symptoms or ECG findings suggested arrhythmia or conduction disturbances, we employed 24-h Holter monitoring. Even in patients without evident arrhythmias, Holter monitoring was routinely performed at one to two years post-procedure to ensure there were no asymptomatic, but clinically significant rhythm disturbances.
All patients were prescribed low-dose acetylsalicylic acid (3 to 5 mg/kg/day) for six months to prevent thromboembolic events during the critical endothelialization phase of the device.
Statistical analysis
Statistical analysis was performed using the IBM SPSS version 26.0 software (IBM Corp., Armonk, NY, USA). Continuous variables were expressed in mean ± standard deviation (SD) or median and interquartile range (IQR), while categorical variables were expressed in number and frequency. Continuous variables were assessed for normality using the Kolmogorov-Smirnov test. For comparisons between antegrade and retrograde approaches, categorical variables were analyzed using the chi-square or Fisher exact test, where applicable. Continuous variables were compared using the Mann-Whitney U test due to non-normal distribution. A cumulative sum (CUSUM) analysis was performed to assess the procedural learning curve. The CUSUM chart was constructed based on the occurrence of procedural failure and major complications which enables the identification of performance trends over time by visualizing deviations from an expected event rate across consecutive cases. A p v alue o f < 0.05 w as considered statistically significant.
Table 1: Demographic characteristic and pre-procedural details of patient
The median procedure duration was 60 (range, 30 to 150) min, and the median fluoroscopy time was 12.6 (range, 6.2 to 43) min. In the initial cases, the antegrade approach was predominantly utilized due to its familiarity and procedural control; however, as operator experience increased, there was a clear shift in preference toward the retrograde method. Consequently, a retrograde approach was employed in 79% of cases, with the 6/4 mm device emerging as the most frequently selected size, as detailed in Table 2. Notably, the retrograde method significantly reduced both procedure duration and fluoroscopy time, underscoring its efficiency advantages (Table 3).
Table 3: Comparison of approaches for transcatheter ventricular septal defect closure
The overall procedural success rate was 95% (55/58). Three cases were considered unsuccessful. In one patient with a history of tetralogy of Fallot surgery, the device embolized into the left pulmonary artery immediately after release due to an insufficient aortic rim, leading to termination of the procedure. Another case involved the development of AV block during the creation of an AV loop using the antegrade approach. The third failed case involved a multifenestrated PMVSD, where the antegrade method was unsuccessful due to entrapment of the tricuspid valve cords, and the retrograde approach revealed a tendency for the device to shift toward the aorta before release.
Complications and follow-up Major complications were observed in three patients (5.4%), including device embolization, AR due to device dislocation, and RV perforation. In one patient with a PMVSD and trivial pre-existing AR, the device had to be surgically removed due to worsening AR within the first postoperative week. Notably, valve repair was not required, and the AR resolved after device removal. Another case involved RV perforation during retrograde defect closure, which resulted in cardiac tamponade. This complication occurred due to excessive contact of the long sheath with the RV apex. In this patient, pericardial fluid was drained surgically, and a small perforation in the RV apex was repaired. In the third case, the device embolized into the left pulmonary artery immediately after release. It was successfully retrieved using a snare, and the VSD was closed with a larger device, resulting in a favorable outcome.
The median follow-up was 34.5 (range, 1 to 56) months. On postoperative Day 1, 23 out of 54 (42%) patients were found to have residual shunts on echocardiography. Among these, 21 patients had minimal shunts (<2 mm), while two patients had moderate shunts (2 to 4 mm). During long-term follow-up, minimal residual shunt persisted in only one patient, indicating that the majority of the residual defects spontaneously resolved over time. Among the 58 patients included in our study, 10 weighed less than 10 kg, and the procedure was successful in all of them, with four exhibiting residual shunts immediately post-procedure. However, during follow-up, all residual shunts resolved completely. During follow-up, new-onset mild tricuspid regurgitation (TR) was observed in one patient, while another patient developed trivial AR in the early postoperative period. By the three-month follow-up, the AR had completely resolved. A patient with a prior history of VSD surgery and minimal AR before the procedure progressed to mild-to-moderate regurgitation. Additionally, one patient developed stenosis in the RV outflow tract with a peak gradient of 29 mmHg post-procedure. By the first-year followup, the stenosis completely resolved, with a gradient reduced to 10 mmHg.
Femoral artery thrombosis occurred in three patients, but Doppler ultrasound at the one-month follow-up revealed normal blood flow in all cases. In one patient, a femoral artery pseudoaneurysm developed, which was successfully treated by thrombin injection, leading to complete resolution. Notably, no cases of complete AV block were reported during follow-up in any patients. However, in the early postoperative period, two patients developed supraventricular tachycardia (SVT), one patient exhibited a nodal rhythm, and two patients experienced incomplete right bundle branch block (IRBBB). While SVT and nodal rhythm returned to normal sinus rhythm, IRBBB persisted in two patients. The Holter ECG was performed on a total of 30 (51.7%) patients. During the third year of follow-up, one patient experienced three episodes of second-degree type 2 AV block, specifically during nighttime sleep, as detected on routine Holter ECG monitoring. Subsequent Holter monitoring revealed no recurrence of AV block, indicating transient conduction disturbances. Detailed complications and follow-up outcomes are summarized in Table 4. A CUSUM chart was constructed to evaluate the procedural learning curve based on the occurrence of procedural failure and major complications. The chart showed a peak during the initial cases, followed by a consistent downward trend after approximately the 10th case, indicating a reduction in serious adverse events as operator experience increased ( Figure 2). This pattern supports the presence of a learning curve in the use of the Konar-MF™ occluder device for transcatheter VSD closure.
Selecting the appropriate device size is critical and should be based on the diameter of the VSD on the RV side, the size of any ventricular septal aneurysm (VSA), the diameter on the LV side, and the size of the aortic rim. Initially, we added a +2 mm margin to the device size on the RV side to ensure complete closure. However, as we gained experience, we adjusted this margin to 0 to 1 mm, optimizing the balance between effective closure and minimizing interference with surrounding cardiac structures. This refined approach led to a reduction in failure rates without a significant increase in residual shunting. In cases with VSA tissue, multiple shunts from different sites of the aneurysm can be observed. Our strategy involved navigating through the largest shunt and positioning the device's waist and LV disc to cover other shunts, allowing us to use a smaller device effectively. This approach aligns with findings from other studies that emphasize the importance of individualized device selection based on anatomical variations.[8, 10]
In our initial use of the Konar-MF™ device, we predominantly utilized the antegrade approach. However, with increasing experience, our preference shifted toward the retrograde method. There were two primary reasons for this transition. First, the retrograde approach resulted in shorter fluoroscopy times and required less manipulation, as it eliminates the need for creating an arteriovenous loop. This reduction in procedural complexity is particularly beneficial in reducing radiation exposure and procedural risks.
Second, the flexible structure of the Konar-MF™ device allows for adjustments during deployment. Even if the left disc does not fully seat within the defect initially, the screw mechanism permits the device to be pushed and positioned precisely into the defect. This capability enables the operator to move the device away from the aortic valve, minimizing the risk of aortic valve interference or regurgitation. The retrograde approach facilitates this maneuverability, providing better control over device placement relative to the aortic valve. This shift in approach aligns with findings from other studies that have highlighted the advantages of the retrograde method when using the Konar-MF™ device;[19, 22] The retrograde implantation method shortens the procedure and fluoroscopy times and offers a safe alternative in cases where creating an AV loop is challenging or poses additional risks, especially in smaller hearts.[23]
Complete AV block is a major concern in transcatheter VSD closure procedures. Early-onset AV block can result from direct trauma caused by the device or delivery system, while late-onset AV block may arise from inflammation, compression, or fibrosis affecting the conduction system. The incidence of AV block following transcatheter VSD closure ranges from 0 to 1% in various studies.[24, 25] In our study, one procedure was terminated without device placement due to complete AV block following AV loop creation. In our practice, severe arrhythmias such as complete AV block or left bundle branch block during transcatheter VSD closure lead us to halt the procedure and deem such cases unsuitable for this approach, a strategy also supported by Tanidir et al.[5] No cases of complete AV block were observed during follow-up, possibly due to the Konar-MF™ device's design, which reduces pressure on the septum and conduction system. However, transient arrhythmias and conduction disturbances occurred in six of 58 patients (10%), primarily during catheter angiography or early postoperatively, resolving spontaneously. Holter ECG was available for 30 patients (51.7%), and second-degree type 2 AV block was observed in one patient during nighttime sleep in the third follow-up year. Control Holter readings for this patient showed no recurrence of AV block.
Valve insufficiency is another significant complication associated with transcatheter VSD closure. Aortic regurgitation may develop if the occluder impinges on the aortic valve leaflets, while TR can occur if the device compresses the chordae tendineae of the tricuspid valve. Studies report the incidence of newly developed TR after transcatheter VSD closure to be between 1 and 9.5%, and newly developed AR between 1 and 5.3%.[24, 25] In our study, newly developing mild AR was observed in one patient (1.8%), which resolved by the third month of follow-up. Another patient required surgical removal of the device due to a gradual increase in AR within the first postoperative week. In cases where the retrograde method was employed, after opening the left disc of the device, we slightly retracted it from the aortic valve using the delivery system before positioning it into the defect. This maneuver helps avoid direct contact with the aortic valve, though it requires careful execution to prevent potential dislocation of the device toward the RV side. Despite our predominant use of the retrograde method, we did not observe a high incidence of aortic valve complications. This may be due to our strategy of selecting smaller-sized devices and adjusting deployment techniques to minimize contact with the valves.
In a meta-analysis, early postoperative residual shunt rates were 15.9%, with permanent residual shunt rates at 1.7%.[25] Haddad et al.[6] reported residual shunt rates of 60% in the early postoperative period, 43% before discharge, and 16% at six months using the Konar-MF™ occluder device. In our study, residual shunt rates were initially 42% on postoperative Day 1, decreasing to 16.6% at six months, 7.4% at one year, and 1.8% at the end of follow-up. This decline over time aligns with findings in the literature, suggesting that many small residual shunts may seal spontaneously during follow-up.[25] Although we adjusted our device selection strategy over time to favor smaller devices when anatomically feasible, this did not lead to an increase in residual shunt rates. Our early postoperative and follow-up residual shunt rates are comparable to those reported in Konar™ studies that employed larger devices based on our strategy.[6, 9] Indeed, our experience demonstrated that selecting smaller devices, particularly in cases with complex anatomy or inadequate aortic rims, allowed us to achieve successful closure without compromising outcomes.
Device embolization is a rare but serious complication, with rates reported between 0 and 5% in studies involving the Konar-MF™ device.[5, 10] In o ur cohort, e mbolization occurred in two (3.6%) patients. One procedure was terminated due to inadequate defect rims, while the other VSD was successfully closed with a larger device after retrieval. Factors contributing to embolization include defect localization, insufficient aortic rims, and improper device selection or technique. The Konar-MF™ device's design allows for either end to be snared, and its softness facilitates easy retraction into the same sheath size used for delivery, which is advantageous in managing such complications. Carminati et al.[2] reported a case of RV perforation during VSD closure with double-disc devices, requiring urgent surgery. While such perforations are not commonly associated with the Konar-MF™ occluder device,[5, 10] we observed this complication in one patient undergoing retrograde VSD closure. It was linked to long sheath manipulation, causing pericardial effusion due to contact with the RV apex. This highlights the importance of careful technique and sheath positioning during the procedure. Analyses performed in the present study demonstrated that failure rates and major complication rates decreased over time with increasing procedural experience. This trend highlights the presence of a learning curve, with improved safety and success as operator proficiency increases. The observed reduction in complications suggests that the procedure can be safely performed, particularly in centers with greater experience.
Nonetheless, there are some limitations to this study. First, this is a single-center, retrospective study. Second, due to the limited number of patients, regression analyses to identify predictors of procedural failure or major complications could not be performed. Following a major complication in the third case, a strategy of selecting smaller devices was adopted; however, the sample size was insufficient to compare this approach with earlier cases where larger devices were used. Additionally, the number of failures and major complications was too small to allow for a meaningful comparison between the antegrade and retrograde approaches. Also, the follow-up period was not sufficient to assess long-term complications. Early cases demonstrated longer procedure times and higher minor complication rates, reflecting the learning curve associated with retrograde deployment. Further multi-center, large-scale, prospective studies with longer follow-up periods are needed to confirm these results.
In conclusion, the Konar-MF™ device offers a viable and safe alternative to surgical ventricular septal defect closure, particularly in younger patients with challenging anatomies. Despite initially higher residual shunt rates postoperatively, these diminish over time, achieving acceptable defect closure proficiency. The design features of the device offer advantages over traditional devices, particularly in reducing the risk of complete atrioventricular block and accommodating anatomical variations. The shift from an antegrade to a retrograde approach, facilitated by increased experience and the device's flexible design, has further optimized procedural outcomes by reducing fluoroscopy times and improving maneuverability during deployment. However, careful assessment is crucial for procedural decision-making, especially in cases of severe arrhythmias during defect closure or insufficient aortic rims that may predispose to embolization. With increasing experience and careful patient and device selection, the success rate is expected to improve, making the Konar-MF™ occluder a viable alternative to surgical ventricular septal defect closure. Ongoing follow-up is essential to monitor for late complications, particularly arrhythmias and changes in valvular function, to ensure long-term patient safety and optimal outcomes. Future studies are warranted to further validate the long-term safety and efficacy of this approach, particularly in high-risk pediatric populations.
Data Sharing Statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions: Conceived of the study, and participated in coordination of study and drafted the manuscript: G.V., M.M.Y., T.M., M.K.; Participated in the design of the study, collection and pocessesing of data: G.V., M.M., C.K., M.B.; Performed the statistical analysis: G.V., M.M.Y.; Involved in general supervision of the research group and reviewed and revised the manuscript: M.M.Y., T.M., M.K. All authors helped to draft the manuscript, read and approved the final manuscript.
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding: The authors received no financial support for the research and/or authorship of this article.
1) Hoffman JI, Kaplan S. The incidence of congenital heart
disease. J Am Coll Cardiol 2002;39:1890-900. doi: 10.1016/
s0735-1097(02)01886-7.
2) Carminati M, Butera G, Chessa M, De Giovanni J, Fisher
G, Gewillig M, et al. Transcatheter closure of congenital
ventricular septal defects: Results of the European Registry.
Eur Heart J 2007;28:2361-8. doi: 10.1093/eurheartj/ehm314.
3) Butera G, Carminati M, Chessa M, Piazza L, Micheletti A,
Negura DG, et al. Transcatheter closure of perimembranous
ventricular septal defects: Early and long-term results. J Am
Coll Cardiol 2007;50:1189-95. doi: 10.1016/j.jacc.2007.03.068.
4) El Said HG, Bratincsak A, Gordon BM, Moore JW. Closure of
perimembranous ventricular septal defects with aneurysmal
tissue using the Amplazter Duct Occluder I: Lessons learned
and medium term follow up. Catheter Cardiovasc Interv
2012;80:895-903. doi: 10.1002/ccd.23074.
5) Tanidir IC, Baspinar O, Saygi M, Kervancioglu M, Guzeltas
A, Odemis E. Use of Lifetech? Konar-MF, a device for both
perimembranous and muscular ventricular septal defects:
A multicentre study. Int J Cardiol 2020;310:43-50. doi: 10.1016/j.ijcard.2020.02.056.
6) Haddad RN, Daou LS, Saliba ZS. Percutaneous closure of
restrictive-type perimembranous ventricular septal defect
using the new KONAR multifunctional occluder: Midterm
outcomes of the first middle-eastern experience. Catheter
Cardiovasc Interv 2020;96:E295-302. doi: 10.1002/ccd.28678.
7) Sadiq M, Qureshi AU, Younas M, Arshad S, Hyder SN.
Percutaneous closure of ventricular septal defect using
LifeTechTM Konar-MF VSD Occluder: Initial and shortterm
multi-institutional results. Cardiol Young 2022;32:755-61. doi: 10.1017/S1047951121002985.
8) Kuswiyanto RB, Gunawijaya E, Djer MM, Noormanto,
Rahman MA, Murni IK, et al. Transcatheter closure of
perimembranous ventricular septal defect using the lifetech
konar-multi functional occluder: Early to midterm results of
the Indonesian multicenter study. Glob Heart 2022;17:15. doi: 10.5334/gh.1106.
9) Kamalı H, Sivaslı Gül Ö, Çoban Ş, Sarı G, Sarıtaş T,
Erdem A, et al. Experiences of two centers in percutaneous
ventricular septal defect closure using konar multifunctional
occluder. Anatol J Cardiol 2022;26:276-85. doi: 10.5152/
AnatolJCardiol.2021.464.
10) Godart F, Baudelet JB, Delarue A, Polge AS, Domanski O,
Bichali S, et al. Transcatheter closure of perimembranous
ventricular septal defects including multifenestrated and
gerbode-type defects using the lifetech konar device. J Clin
Med 2023;12:6370. doi: 10.3390/jcm12196370.
11) Holzer R, de Giovanni J, Walsh KP, Tometzki A, Goh T, Hakim
F, et al. Transcatheter closure of perimembranous ventricular
septal defects using the amplatzer membranous VSD
occluder: Immediate and midterm results of an international
registry. Catheter Cardiovasc Interv 2006;68:620-8. doi: 10.1002/ccd.20659.
12) Predescu D, Chaturvedi RR, Friedberg MK, Benson LN,
Ozawa A, Lee KJ. Complete heart block associated with
device closure of perimembranous ventricular septal defects.
J Thorac Cardiovasc Surg 2008;136:1223-8. doi: 10.1016/j.
jtcvs.2008.02.037.
13) Nguyen HL, Phan QT, Doan DD, Dinh LH, Tran HB,
Sharmin S, et al. Percutaneous closure of perimembranous
ventricular septal defect using patent ductus arteriosus
occluders. PLoS One 2018;13:e0206535. doi: 10.1371/journal.
pone.0206535.
14) Chungsomprasong P, Durongpisitkul K, Vijarnsorn C,
Soongswang J, Lê TP. The results of transcatheter closure
of VSD using Amplatzer® device and Nit Occlud® Lê coil.
Catheter Cardiovasc Interv 2011;78:1032-40. doi: 10.1002/
ccd.23084.
15) Haas NA, Kock L, Bertram H, Boekenkamp R, De Wolf D,
Ditkivskyy I, et al. Interventional VSD-Closure with the Nit-Occlud® Lê VSD-Coil in 110 patients: Early and midterm
results of the EUREVECO-Registry. Pediatr Cardiol
2017;38:215-27. doi: 10.1007/s00246-016-1502-8.
16) Yang J, Yang L, Wan Y, Zuo J, Zhang J, Chen W, et al.
Transcatheter device closure of perimembranous ventricular
septal defects: Mid-term outcomes. Eur Heart J 2010;31:2238-45. doi: 10.1093/eurheartj/ehq240.
17) Zhou D, Pan W, Guan L, Ge J. Transcatheter closure of
perimembranous and intracristal ventricular septal defects
with the SHSMA occluder. Catheter Cardiovasc Interv
2012;79:666-74. doi: 10.1002/ccd.23344.
18) Mandal KD, Su D, Pang Y. Long-term outcome of transcatheter
device closure of perimembranous ventricular septal defects.
Front Pediatr 2018;6:128. doi: 10.3389/fped.2018.00128.
19) Muthusamy K. Retrograde closure of perimembranous
ventricular septal defect using muscular ventricular septal
occluder: A single-center experience of a novel technique.
Pediatr Cardiol 2015;36:106-10. doi: 10.1007/s00246-014-0971-x.
20) Koneti NR, Penumatsa RR, Kanchi V, Arramraj SK, S
J, Bhupathiraju S. Retrograde transcatheter closure of
ventricular septal defects in children using the Amplatzer
Duct Occluder II. Catheter Cardiovasc Interv 2011;77:252-9.
doi: 10.1002/ccd.22675.
21) Morray BH. Ventricular septal defect closure devices,
techniques, and outcomes. Interv Cardiol Clin 2019;8:1-10.
doi: 10.1016/j.iccl.2018.08.002.
22) Haddad RN, Saliba ZS. Comparative outcomes of
two competitive devices for retrograde closure of
perimembranous ventricular septal defects. Front Cardiovasc
Med 2023;10:1215397. doi: 10.3389/fcvm.2023.1215397.
23) Jiang D, Zhang J, Fan Y, Han B, Zhao L, Yi Y, et al. The
efficacy and medium to long-term follow-up of transcatheter
retrograde closure of perimembranous ventricular septal
defects via the femoral artery with amplatzer duct occluder
II in children. Front Pediatr 2021;9:571407. doi: 10.3389/
fped.2021.571407.


Turkish Journal of Thoracic and Cardiovascular Surgery published orginal papers on topics in cardiovascular surgery, cardiovascular anesthesia,cardiology and thoracic surgery. These encompass all relevant clinical, surgical and laboratory specialities, editorials, current and collective reviews, tecnical knowhow papers, case reports, "How to Do It" papers. All copyrights of the articles that published or will be published belongs to Turkish Journal of Thoracic and Cardiovascular Surgery and without permission of editorial board whole articles or any part of articles table pictures and graphics could not be published. Turkish Journal of Thoracic and Cardiovascular Surgery is indexed by Science Citation Index - Expanded (SCIE)
Editor of the Journal of Turkish Thoracic and Cardiovascular Surgery
Ataşehir Mah. Ataşehir Bulvarı 48 Ada Mimoza 2-2 K:2 D:6 Ataşehir - İSTANBUL - TURKEY
Phone: +90 216 456 14 54 | GSM: 0549 456 14 54 | e - Mail : dergi@tkdcd.org
www.tkdcd.org

){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}